Why hasn’t there been more progress in medical technology?
During late night college musings with friends two decades ago, three interconnected ideas dominated our thinking: (1) Humans would live twice as long, (2) There would be a renaissance of ideas, since every inch of the planet would have have internet access, and (3) Computing power would be effectively free, giving rise to advanced artificial intelligence.
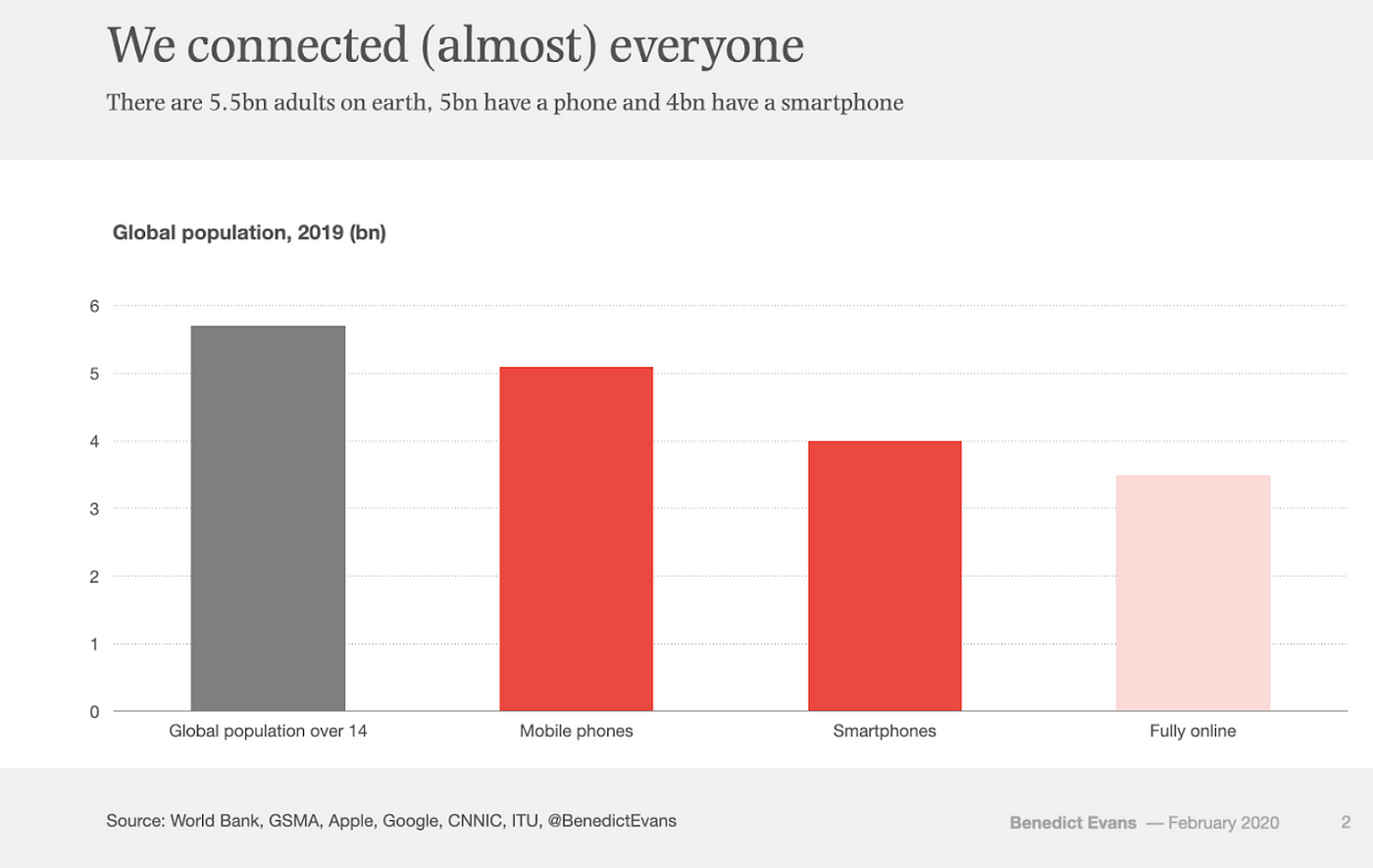
With respect to (2), though I now appreciate the limitations of global internet coverage (RIP to OneWeb), we’ve done remarkably well on internet access. As Ben Evans highlights in the chart, 90% of adults on the planet have a mobile phone and 80% are fully online. A huge driver has been the rapid decline in global extreme poverty: in 1990, over a third of the world lived in extreme poverty; in 2015, that rate had dropped to 10%, via World Bank. If you think the world is going to hell in a hand-basket, consider that incredible stat.
Even accounting for the din of polarization on social media, how amazing is it that so many people have instant access to scientific research, Wikipedia, and MIT OpenCourseware? The full “renaissance” may take a generation, but it’s hard to imagine that free information won’t give rise to better, richer, more inclusive ideas.
For (3), the cloud has made computing accessible to anyone, enabling advanced AI. With a credit card on AWS, Descartes Labs made it to the TOP500 supercomputer list in 2019, something that would have cost millions of dollars worth of physical hardware just a few years earlier. Though we still have a long way to go with AI, our strides there have been impressive and have improved our lives.
However, this post is not about software or hardware, it’s about medicine.
Just a few weeks ago, I was stuck in the hospital with an infection—not COVID-19, and I’m much better now, thank you. It was a stark reminder both how incredible medicine is and how far we have to go.
For example, after an ultrasound of my heart, it appeared as though I had a vegetation (i.e., infection) on one of my aortic valves. If I had an infected vale, open heart surgery would have been certain. My options would have been to replace with an artificial valve, which would require blood thinners; or a valve from my own tissue, which would fail after a decade. After a more advanced test involving a camera being shoved down my throat, it was discovered that I have a congenital defect, a bicuspid valve. Something to watch, but nothing to worry about until later in life.
I’m thankful that I actually was fine and, even if I had issues, there were plenty of options. How cool is it that we can install an artificial valve?
On the other hand, imagine this future: my mother knows that I had a bicuspid valve before birth, thanks to a DNA test. Because I have a quick, harmless full body scan every year, my doctors can easily monitor my valve and detect any other emerging problems. Infections are caught early, thanks to daily monitoring of my blood. My immune system is constantly augmented by personalized molecules to ensure I never get sick. And, because doctors have so much data on bodies, studies are able to be done at scale, greatly accelerating medical science. Heck, I even get personalized recommendations for what to eat to keep my diet in check.
Though I’m demonstrating both a lack of creativity (too narrow) and lack of understanding about medicine (imagining things that are impossibly hard), the question still remains: how do we greatly accelerate medical science?
With coronavirus ravaging lives and economies, the question is more pertinent than ever. 75% of venture goes to software, whereas only about 10% goes to biotech according to an article MIT Tech Review, “Why doesn’t venture capital build the things we need?” With the current zeitgeist, the article focuses on what type of people get funded, rather than the structures that give rise to funding decisions.

The chart above shows that more money is going into biotech, but how do we increase that number by 10x or 100x? How do we get a cure for cancer before you, dear reader, succumb to it.
The answer is complicated and I can’t get it out of my head. Let me offer a few ideas.
Doctors aren’t (typically) entrepreneurs—doctors receive enormous amounts of training—medical school, residency, sometimes a fellowship—and are focused on saving patients, not on imaging how to build a company. At my last startup, we used to joke about “jailbreaking” scientists from labs to make them far more productive and useful. Perhaps we need to jailbreak some doctors.
Geeks don’t understand wetware—many readers of this post will deeply understand hardware and software, but only have a minimal understanding of chemistry and biology. The paradigms of chemistry are very different from the world of 1s and 0s. I’m certainly in that camp, so I started a (free internet) course on biology (from a top university) to get familiar. Software indeed has eaten the world.
Too much regulation—investing in biotech means allocating a huge percentage of your startup dollars to regulatory red tape. That deters investment, because investors want capital to go to product, not lawyers. The regulatory framework is enormously complex. An example affecting us right now: coronavirus vaccines look promising exactly because the FDA has “set the regulatory stage for drug and biologics manufacturers to develop products” according to FDA commissioner Hahn. Why should it take a global pandemic to update regulation?
Messy incentive structures—as with any core research, the right funding framework should be in place to encourage R&D to see the light of day. Bell Labs created innovations that capital markets eventually funded. Healthcare is difficult because there’s some notion that no one should profit on saving lives. Even the WSJ insinuates that investors could profit if Oxford wins the coronavirus battle, as if that’s a bad thing. The profit motive should be encouraged, as it will drive innovation and attract capital.
Data is not available at scale—key to improving medicine is collect huge amounts of data. Whether that data is used for personal recommendations on diet and exercise or whether it’s used for advanced longitudinal studies, we need it more than ever. Just look at the sorry state of coronavirus modeling for evidence that, whereas FANG is awash with continuous data, medical science is left with poor sampling. Data refineries need to become as common in the world of medicine as they are in Big Tech.
Government funding is too low—why, oh why, did not the United States stand up at the beginning of coronavirus and announce a Manhattan Project for health? Certainly figuring out how to deliver healthcare to all Americans is important and is a huge, hairy, messy problem. Concurrently, we ought to throw money into R&D to eliminate a huge number of healthcare issues. If we allocate dollars towards improving the quality and length of our lives, we can potentially bring down healthcare costs, making universal healthcare tractable.
As I start learning more about medical technology, what should I be thinking about? What problems did I miss?
